
Danniel Martinez
Verified Author
Dr. Sarah Chen, MD, PhD
Neurologist & Cognitive Researcher
Introduction
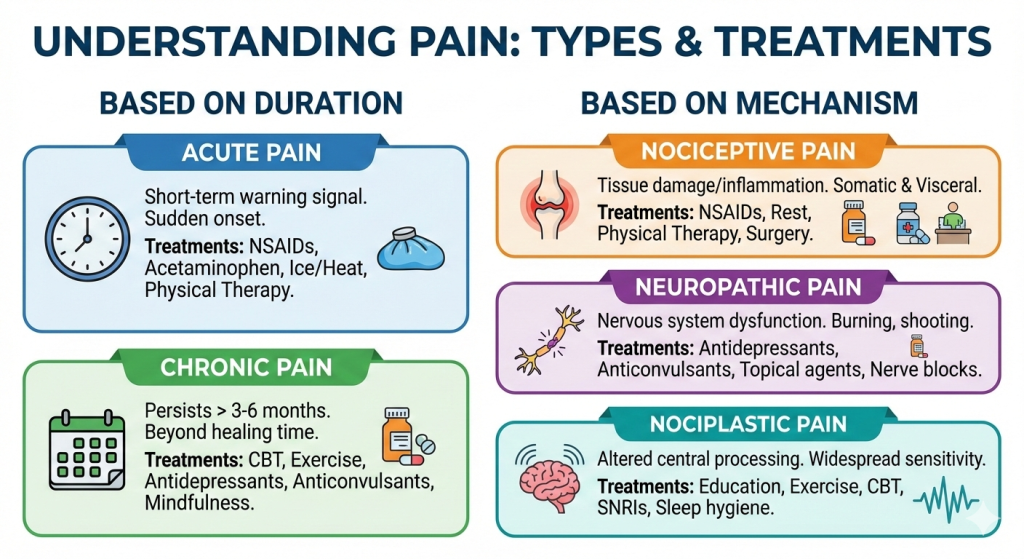
Finding out what kind of pain you have can help you get better relief. Pain can be anything from sharp stabs after an injury to aches that won’t go away from fibromyalgia. Twenty to thirty percent of people around the world and twenty-four percent of adults in the U.S. have chronic forms. This guide lists types of pain: acute, chronic, nociceptive, neuropathic, and nociplastic. It also lists specific treatments, such as medications and therapies. The CDC and IASP guidelines will give you concrete strategies to discuss with your doctor. With knowledge, you can avoid needless pain.
What Is Pain?
When you get hurt, pain tells you to protect yourself, like the sting of a cut. IASP, the International Association for the Study of Pain, says that pain is “an unpleasant sensory and emotional experience associated with actual or potential tissue damage.” Somatic (skin, muscles), visceral (organs), and referred (felt elsewhere) are some of the different forms. The rate rises with age, and 8% of adults can’t do anything because of high-impact chronic pain. Knowing the type helps you decide whether it’s temporary or long-lasting, leading you to rest or to specialists.
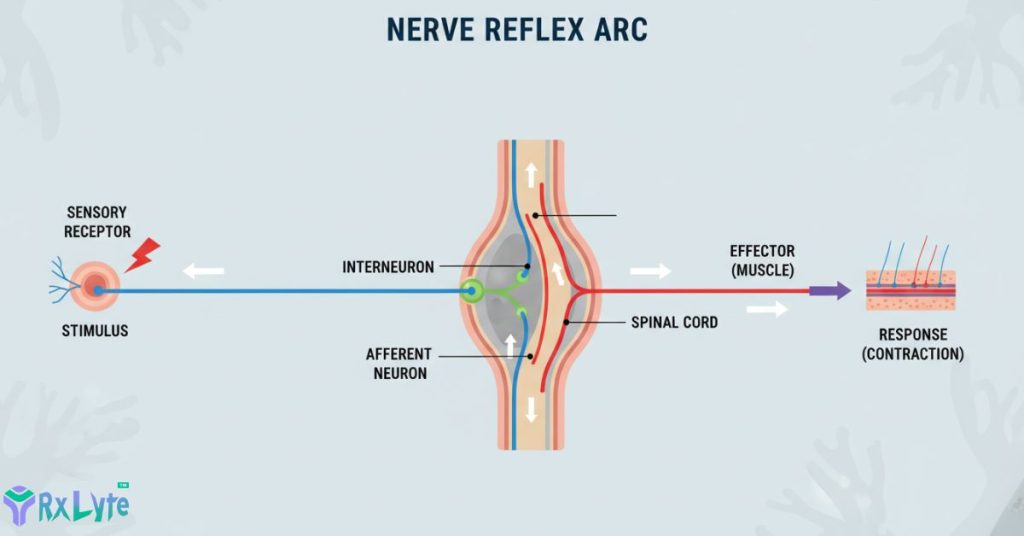
How do the pathways of pain work?
Nociceptors are nerve endings that transmit signals to the brain via the spinal cord when they detect heat, pressure, or chemicals. It’s like a smoke alarm chain: damage triggers prostaglandins, which make the alarm louder. Acute signals go away as the body heals, but chronic ones glitch and cause looping hypersensitivity. The effects happen quickly—in seconds for touch—making you want to stop. Parts of the brain, like the amygdala, make us feel emotions, which is why stress makes them worse. The treatments go after these paths: NSAIDs stop chemicals from working, and gabapentinoids calm nerves.
Acute Pain
Acute pain comes on quickly after an injury or surgery and lasts for less than 3 months, helping protect the body. Sharp, localized throbs can be caused by sprains, burns, or dental work. In contrast to chronic, it makes you want to rest and goes away when you heal. The CDC says it works best with non-opioids first. Most people get it after an accident, and they don’t leave scars. To help with a quick recovery, your doctor may tell you to take ice with your medicine.
Chronic Pain
Chronic pain lasts longer than three months, like a fire alarm that stays on all the time. It affects 24.3% of adults in the U.S., most often because of back or arthritis problems. Unlike acute, it wears down nerves and makes both physical and emotional pain worse. The WHO ladders for non-opioids indicate that multimodal care works really well here. After the pandemic, rates went up, which made it very hard. The tailor comes closer; persistence indicates that more checks are needed.
Nociceptive Pain
The pain we feel is caused by damaged tissue, and our nociceptors detect real threats. Visceral pain affects organs (cramping) and somatic pain affects bones and muscles (dull aches). Often seen in broken bones or appendicitis. Increases prostaglandins and swelling at sites of inflammation. It fades with repair. NSAIDs or acetaminophen work well to target it and stop signals early. Set them apart by their sharpness to the touch.
Neuropathic Pain
Neuropathic pain occurs when nerves are damaged or don’t work properly, sending out incorrect signals like crossed wires. Burning, tingling, and electric shocks can be caused by diabetes, shingles, or chemotherapy. Central (spinal) or peripheral types numb or make the nerves more sensitive. Not like nociceptive, there is no damage. In tests, first-line drugs like duloxetine calm it down 30–50%. As neuropathy epidemics spread, the number of cases rises.
Nociplastic Pain
Nociplastic pain speeds up brain activity without hurting nerves or doing any damage—a hypersensitive volume knob. Fibromyalgia is an example of widespread pain and tiredness. IASP rates it based on signs such as allodynia, in which light touch hurts. No clear triggers; stress gets worse. NICE says that exercise and cognitive-behavioral therapy (CBT) are more effective than some medications. It covers other things, so it needs a whole-person view.
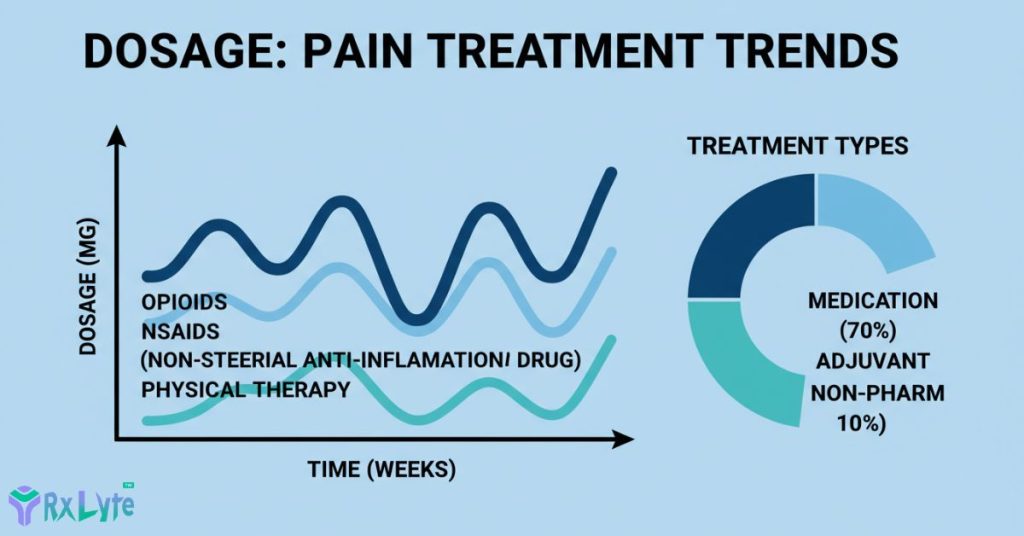
Uses and benefits of medicine
NSAIDs and acetaminophen are used to treat nociceptive and acute pain, and they reduce inflammation by 50% or more. Neuropathic patients like gabapentinoids and SNRIs, which lower pain scores by 40%. Intensity should be cut by 20 to 30 percent for neuroplastic and chronic pain. TENS and acupressure are non-drug ways to boost. There is evidence that multimodal therapy cuts disability in half compared to medication alone. Opioids are only used as a last resort in cases that don’t respond to other treatments.
Dosage and Administration
Doses change; your doctor makes changes. Take with food and at the right time.
| Acetaminophen | Nociceptive/Acute | 500-1000mg every 6h | 4000mg | Water, anytime |
| Ibuprofen (NSAID) | Nociceptive/Acute | 400mg every 6h | 2400mg | With food |
| Gabapentin | Neuropathic | 300mg/day, | 3600mg | Slow ramp-up |
| Pregabalin | Neuropathic | 150mg/day | 600mg | Split doses |
| Duloxetine | Neuropathic/Nociplastic | 30mg/day | 60mg | Morning |
| Amitriptyline | Neuropathic | 10-25mg nightly | 150mg | Bedtime |
Read labels and reevaluate every week.
Health Risks and Side Effects
Closely watch; most are mild, but keep an eye on patterns.
Common Side Effects
Benzodiazepines (20%) cause dizziness, SNRIs (15%) cause nausea, and TCAs cause dry mouth.
Serious Side Effects
Thoughts of suicide (SNRIs and TCAs), swelling (pregabalin), and serotonin syndrome. For trouble breathing or confusion, call a doctor.
Rare Adverse Reactions
allergens, hallucinations; liver strain is rare if you keep an eye on it.
Important: If you get a rash or swelling, stop and get help.
Cautionary Notes and Not Recommended
Never take TCAs for glaucoma or gabapentinoids for kidney failure. If you are pregnant, you should not take high doses of SNRIs. Topical SNRIs are safer. For sensitive people over 65, half the dose. These conditions make NSAIDs less safe. Kids need help from pediatricians.
How Drugs and Supplements Work Together
While duloxetine interacts with MAOIs, gabapentinoids make opioids more sedating. Alcohol makes feeling dizzy worse. Swelling from St. John’s Wort is possible. It changes how pregabalin works. Tell your pharmacist about herbs.
Dos and Don’ts
- Put chronic types on medicine and get them moving.
- Keep a pain diary every day.
- Stay well hydrated while taking SNRIs.
- Tapering gabapentinoids should not be done all at once.
- For acute pain relief, mix heat and ice.
- Do not drink any alcohol.
- Keep medicines at room temperature.
- Ignore non-drug things like yoga? Not at all—type in nociplastic.
- Look at the location and intensity.
- Note what sets it off (touch? Night?).
- First, try something that isn’t a drug.
- If you need to, add med.
- Check back in a week.
Tip: Keep pain logs on apps and share them with doctors.
When You Should See a Doctor
Pain that changes type, spreads, or is accompanied by weakness or fever may indicate nerve compression. In emergencies, the pain is sudden and severe, and it’s linked to the chest. Chronic not helped? Multimodal plan for follow-up. Screenings for diabetics once a year can stop neuropathic pain from getting worse.
Conclusion
Pain types, ranging from sharp throbs to a hazy, nociplastic haze, need different treatments, such as NSAIDs, gabapentin, or PT. Multimodal wins because it lowers risks and increases life. Talk to your healthcare provider before making any changes. You know how you feel best—partner for wins.
Frequently Asked Questions
Nociceptive pains are dull or sharp and come from injury. Neuropathic pains are burns or tingles that have no cause. History and tests from the doctor confirm. Start with drugs that aren't opioids.
Yes, IASP and NICE say that graded activity does lower sensitivity. Add CBT; medications come second. For a safe start, talk to PT.
Strong advice from the CDC: use ice and NSAIDs (topical or oral) or acetaminophen. Not unless it's really bad.
Slowly titrate; keep an eye on the kidneys. Good for neuropathic pain, but taper off slowly to avoid withdrawal. Key to doc oversight.
There isn't a lot of evidence that capsaicin creams help neuropathic pain. Talk about it before you add.
When used alone, medications don't work as well as PT/psych. Adapts to your profile.
0 Comments