
Danniel Martinez
Verified Author
Dr. Sarah Chen, MD, PhD
Neurologist & Cognitive Researcher
One of the most popular types of medicine in the world is nonsteroidal anti-inflammatory drugs (NSAIDs). Every day, millions of people take ibuprofen, naproxen, or diclofenac to treat pain and inflammation. The National Centre for Biotechnology Information says that NSAIDs are prescribed to treat pain, fever, and inflammatory processes that can be caused by everything from arthritis to headaches. Even though these three common NSAIDs work in similar ways, knowing how they differ in strength, duration, side effects, and the right way to use them can help you make better decisions about how to manage your pain. This complete guide explains how ibuprofen, naproxen, and diclofenac work, when to use each, and important safety tips to help prevent serious side effects.
What Are NSAIDs?
There is a group of medicines called nonsteroidal anti-inflammatory drugs that can help with pain, fever, and inflammation without containing steroids. “Nonsteroidal” makes them different from corticosteroids like prednisone, which work in very different ways and have very different sets of side effects. NSAIDs work by stopping certain enzymes from making prostaglandins. Prostaglandins are chemical messengers that trigger pain, inflammation, and fever.
What Makes NSAIDs Different from Other Painkillers
NSAIDs act on inflammation in both the central and peripheral nervous systems. In contrast, acetaminophen (paracetamol) primarily acts in the central nervous system to reduce pain and fever, with minimal anti-inflammatory effects. Because of this, NSAIDs work especially well for conditions like arthritis, sports injuries, dental pain, and menstrual cramps, where inflammation makes pain worse. NSAIDs are also not the same as opioid painkillers, which work by attaching to opioid receptors in the brain and spinal cord. Opioids may be better at relieving severe pain, but NSAIDs are better at managing mild to moderate pain and don’t have the tendency to become addictive or make you sleepy like opioids do.
NSAIDs come in two types: selective and non-selective.
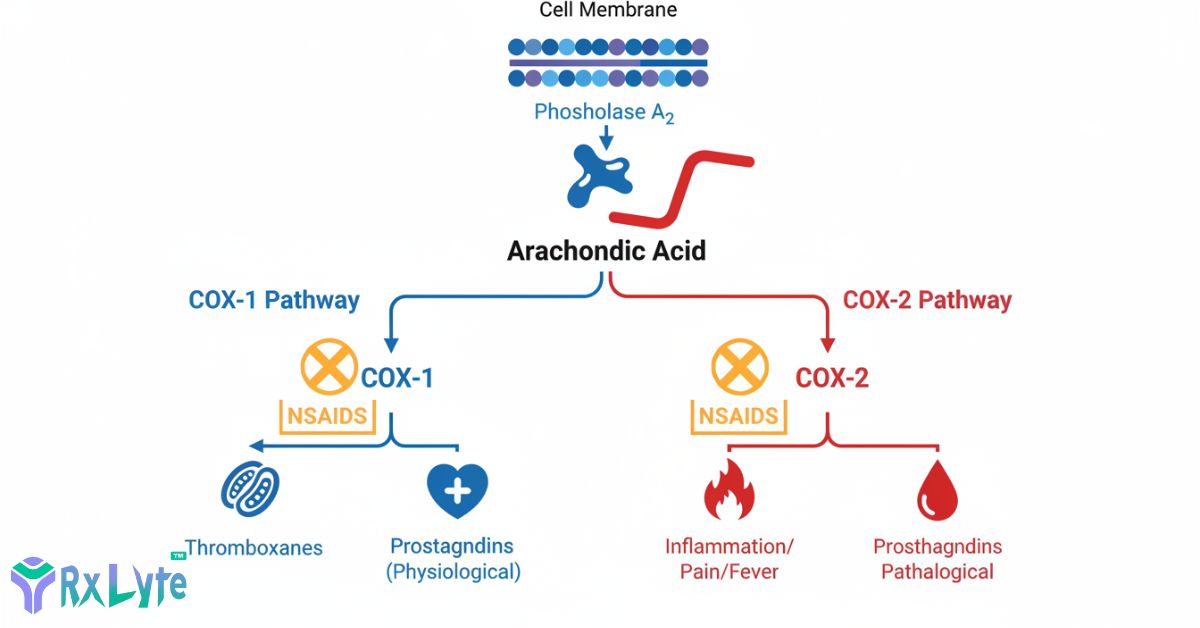
Based on which enzymes they block, NSAIDs can be put into two main groups. Non-selective NSAIDs, such as ibuprofen, naproxen, and diclofenac, inhibit both COX-1 and COX-2. COX-1 enzymes clean up your body by doing things like protecting the lining of your stomach and helping your kidneys work. COX-2 enzymes, on the other hand, are mostly responsible for inflammation and pain responses. Celecoxib and other selective COX-2 inhibitors target only COX-2 enzymes, which should reduce the risk of stomach problems. Medical journal research, on the other hand, shows that all NSAIDs, selective or not, have risks for the heart and stomach that need to be carefully thought through.
How do NSAIDs do their job?
NSAIDs work as painkillers by messing with your body’s inflammatory cascade. This is a complicated set of chemical reactions that happen when your body is dealing with tissue damage, infection, or long-term conditions. Being aware of this process helps explain both the advantages and possible disadvantages of using NSAIDs.
The COX System of Enzymes
Two kinds of cyclooxygenase (COX) enzymes are made by cells when they are hurt or inflamed: COX-1 and COX-2. These enzymes change arachidonic acid, a fatty acid found in cell membranes, into prostaglandins. Prostaglandins amplify pain signals, raise body temperature, and cause injury sites to swell. National Institutes of Health research shows that NSAIDs can temporarily stop both COX-1 and COX-2 enzymes from working. This stops the production of prostaglandin precursors. Blocking the production of prostaglandins eases pain and lowers inflammation. Still, it also prevents protective prostaglandins from doing their job, which helps keep the stomach lining strong, kidney blood flow in check, and platelets working properly.
NSAIDs lower fever, pain, and swelling because
NSAIDs stop multiple pathways at the same time by stopping the production of prostaglandins. To ease pain, lower levels of prostaglandin make nerve endings less sensitive at injury sites and stop pain signals from getting to your brain. When you take an antipyretic, your body’s temperature drops because prostaglandins are turned off in the hypothalamus, which is the temperature control centre of your brain. Reducing prostaglandin-mediated vasodilation (blood vessel widening), vascular permeability (fluid leakage into tissues), and inflammatory cell recruitment to affected areas helps reduce inflammation. Some other ways it works include stopping chemotaxis, altering lymphocyte activity, and lowering levels of proinflammatory cytokines, but these mechanisms are not fully understood either.
The most common NSAID is ibuprofen.
Ibuprofen is the most well-known and widely used NSAID in the world. It can be bought over the counter in a variety of forms, including tablets, chewable tablets, liquid suspensions, and topical preparations. Because it is easy to get, has a well-known safety profile at recommended doses, and works quickly, it is often the first choice pain reliever for many conditions.
Medical Uses and How Well They Work
Ibuprofen is recommended by doctors to treat several painful and inflammatory conditions. Osteoarthritis, rheumatoid arthritis, dysmenorrhea (menstrual cramps), mild to moderate pain from headaches or dental procedures, lowering fevers, and acute musculoskeletal injuries are the main reasons why this medicine is used. Ibuprofen has been shown to help with short-term pain, but research published in Arthritis Research & Therapy suggests it may not be as good for chronic arthritis pain as some other NSAIDs. Within 30 to 60 minutes, the medicine starts to work, making it good for temporary pain relief.
How Much Ibuprofen Should You Take?
Dosing for over-the-counter and prescription ibuprofen is very different, according to FDA-approved prescribing information:
Ibuprofen without a prescription:
- Two hundred to four hundred mg every four to six hours, or as needed.
- Most that can be taken in one dose is 400 mg (without medical supervision).
- Every day, the most you can take is 1,200 mg.
Ibuprofen with a prescription:
- Every day, take 400 mg, 600 mg, or 800 mg three to four times.
- No more than 3,200 mg per day for adults.
- Different dosing schedules may be needed for different conditions.
Most prescriptions for osteoarthritis and rheumatoid arthritis range from 300 mg four times a day to 800 mg three to four times a day. For dysmenorrhea, 400 mg every four hours is usually enough. To keep side effects to a minimum, always take the lowest effective dose for the shortest time possible to control your symptoms.
How Long Does an Action Last?
The half-life of ibuprofen is about 2 hours, but its effects usually last 4 to 6 hours. Because ibuprofen doesn’t last as long as some other NSAIDs, you’ll have to take it more often during the day if you need to keep the pain under control. It takes about an hour or two for the medicine to reach its peak in the blood, meaning it is working at its strongest to relieve pain. Ibuprofen is broken down in your liver, and the main way it leaves your body is through your kidneys. This shorter duration has pros and cons. Merely taking the medicine more often may be inconvenient, but it leaves your body faster, which can be helpful if you have side effects or need to switch medicines.
Naproxen: The Choice That Lasts Longer
Naproxen, which is sold over the counter under the brand name Aleve, works longer than ibuprofen, which makes it great for conditions that need pain relief all day or night. The National Centre for Biotechnology Information says that naproxen is the first drug that should be used to treat acute gouty arthritis, osteoarthritis, musculoskeletal pain, inflammation, and menstrual problems.
Medical Uses and How Well They Work
Acute gout, ankylosing spondylitis, bursitis, polyarticular juvenile idiopathic arthritis, osteoarthritis, tendonitis, rheumatoid arthritis, pain, and primary dysmenorrhea are all conditions for which the FDA has approved naproxen to treat. Doctors often prescribe naproxen for people with chronic inflammatory conditions because it lasts longer than ibuprofen and only needs to be taken twice a day instead of three to four times a day. Even though naproxen and other NSAIDs work well to treat inflammatory arthropathies, they don’t stop the disease from getting worse or stop the damage that these conditions cause to joints and soft tissues. The pain-relieving effects of naproxen start in 30 to 60 minutes, which is about the same time as ibuprofen.
How Much Naproxen Should You Take?
Naproxen comes in both over-the-counter and prescription strengths, and the right dose depends on the type of drug and the reason for taking it.
Aleve, which is over-the-counter naproxen sodium:
- Every 8 to 12 hours, you should take 220 mg.
- The most you can take in a day is 660 mg, which is three tablets.
- If you want to avoid stomach upset, take it with food or milk.
Naproxen with a prescription:
- How much to take: 250 mg to 500 mg twice a day
- The most that can be taken in a day is 1,500 mg, which can be split into two doses of 500 mg and 250 mg every 6 to 8 hours.
- Extended-release types: 375 mg to 500 mg once or twice a day
About 95% of naproxen is flushed out of the body in the urine after being broken down by the liver. People who have problems with their kidneys or liver may need to change their doses so that drugs don’t build up and cause more harm.
This is why naproxen lasts longer.
The fact that naproxen has a much longer half-life than ibuprofen means that it works for a longer time. Medical pharmacology data show that naproxen is eliminated from the body between 12 and 17 hours in adults whose kidneys work normally. Because it has a longer half-life, naproxen stays in your bloodstream for a much longer time. This means that it can relieve pain for up to 12 hours. Peak levels of naproxen in the blood happen 2 to 4 hours after taking regular naproxen tablets or 1 to 2 hours after taking naproxen sodium formulations. More than 99% of the drug binds to albumin proteins in your blood. This makes a reservoir that releases the active drug slowly over time. For people who need to manage their pain all the time, naproxen’s longer duration often means better medication compliance and more consistent symptom control.
Diclofenac: The Choice for Prescription Strength
Diclofenac is one of the strongest NSAIDs on the market. Because of its strength and risk profile, it usually needs a prescription in most countries. Medical journal research shows that diclofenac is more effective than ibuprofen. This makes it a better choice for conditions that need stronger anti-inflammatory effects.
Medical Uses and How Well They Work
The main reasons doctors give diclofenac are to treat osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, acute pain, dysmenorrhea, and migraines. A study from Arthritis Research & Therapy looked at many studies and found that oral diclofenac, especially at 150 mg per day, helped with arthritis pain more than celecoxib, naproxen, and ibuprofen (NSAIDs). Because it is stronger, diclofenac is especially helpful for people who haven’t been able to get enough pain relief from over-the-counter NSAIDs. The increased effectiveness does, however, come with a higher risk of both gastrointestinal and cardiovascular side effects.
How Much Diclofenac Should You Take?
Diclofenac comes in a number of different forms, and the way it should be taken depends on the condition being treated:
Oral Diclofenac:
- Joint pain: 50 mg twice or three times a day, or 75 mg twice a day
- RA: 50 mg twice or three times a day, or 75 mg twice a day
- Ankylosing spondylitis: 25 mg four times a day, plus an extra 25 mg before bed if needed
- For menstrual pain, take 50 mg three times a day.
- Pain level 1 to 2: 50 mg three times a day
- The most you can take in a day is 150 mg.
Topical Diclofenac:
- For knee osteoarthritis, put 40 mg (2 pump actions) on the knee 4 times a day.
- Cover the front, back, and sides of the hurt joint evenly.
- Maximum amount put on the skin: 32 grams per day for all joints that are being treated
Topical formulations let you put the medicine directly on painful joints, which may lower the drug’s systemic exposure and side effects while still providing anti-inflammatory benefits locally.
Use of Topical vs. Oral Formulations
Diclofenac comes in both oral and topical forms, which gives doctors more options for how to treat patients. Diclofenac gel or solution that is applied topically can be put directly on joints that hurt, like knees, hands, or feet that have osteoarthritis. When the medicine is given this way instead of by mouth, it lowers the amount in the blood, which should lower the risk of systemic side effects like stomach bleeding or heart problems. Topical NSAIDs, on the other hand, may cause redness, itching, or rashes on the skin where they are applied. Oral diclofenac comes in three different forms: immediate-release, delayed-release, and extended-release. Each type is made for a different release pattern and dosing schedule. Delayed-release tablets keep the medicine safe from stomach acid. The medicine is released in the small intestine, which may help soothe the stomach.
Ibuprofen, Naproxen, and Diclofenac Side-by-Side Comparison
This information about the main differences between these three common NSAIDs will help you and your doctor choose the best one for your needs, taking into account safety, effectiveness, and ease of use.
Differences in Potency
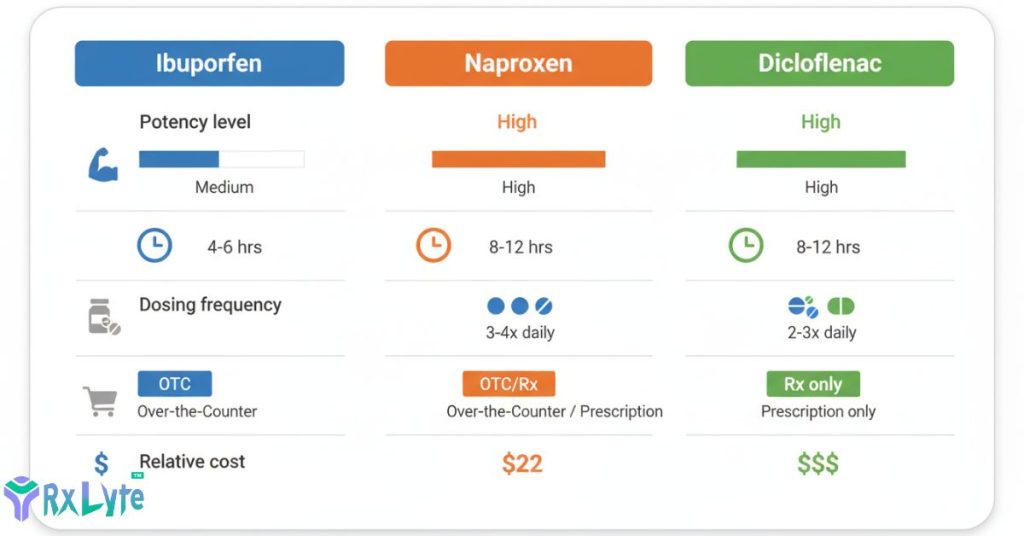
Researchers have found clear differences in how strong these three NSAIDs are compared to each other. Studies on people have shown that diclofenac is the strongest pain reliever, followed by naproxen. Ibuprofen is the weakest of the three. In other words, smaller amounts of diclofenac relieve pain just as well as larger amounts of naproxen or ibuprofen. For people with long-term inflammatory conditions like rheumatoid arthritis or severe osteoarthritis, the difference in potency may be especially important because stronger anti-inflammatory effects may mean better symptom control. But stronger drugs come with higher risks. For example, studies show that diclofenac has about four times the normal risk of gastrointestinal bleeding and heart problems compared to ibuprofen, which has about two and a half times the normal risk of gastrointestinal bleeding.
Duration of Relief
| NSAID | Half-Life | Duration of Effect | Typical Dosing Frequency |
|---|---|---|---|
| Ibuprofen | ~2 hours | 4-6 hours | Every 4-6 hours (3-4 times daily) |
| Naproxen | 12-17 hours | 8-12 hours | Every 8-12 hours (1-2 times daily) |
| Diclofenac | 1-2 hours (standard); up to 12 hours (extended-release) | 8-12 hours | 2-3 times daily (standard); 1-2 times daily (extended-release) |
Taking painkillers often or all night long is not an option. Ibuprofen’s shorter half-life may be helpful if you need the drug to leave your body quickly, like before surgery or if you are having side effects.
Availability and Cost
Different medications are harder to get and cost more or less:
- Ibuprofen is widely available over-the-counter in strengths up to 400 mg per tablet. Prescription versions (600 mg and 800 mg) are also available, and it is usually the cheapest option.
- Naproxen: You can buy naproxen sodium (Aleve, 220 mg) over-the-counter, and stronger prescription versions are also available. It is a moderately priced drug.
- Most countries require a prescription to get diclofenac, but some topical forms may be sold without a prescription. It is usually more expensive, especially for brand-name products.
All three medicines are available in generic forms that are much cheaper than their brand-name counterparts while still being just as effective and safe.
Adverse effects and worries about safety

Anti-inflammatory drugs (NSAIDs) are good at relieving pain and inflammation, but they also come with serious risks that get worse with higher doses, longer use, and some personal risk factors. Concerns about heart disease and stomach problems have been raised by the FDA in boxed warnings for all NSAIDs.
Common Effects
Publicly available medical research shows that 10% to 60% of people who take NSAIDs may experience minor side effects. Common responses are:
- Nausea and upset stomach
- Dyspepsia (indigestion)
- Abdominal pain or discomfort
- Heartburn or acid reflux
- Diarrhea or constipation
- Flatulence (gas)
- Dizziness or headache
- Mild drowsiness
Most of the time, these effects go away on their own or get better when you take the medicine with food. If minor side effects last longer or get worse, talk to your doctor about other ways to deal with pain.
Serious Risks for Heart Disease
NSAIDs raise the risk of serious heart problems like myocardial infarction (heart attack), stroke, and heart failure, according to research published in medical journals. The FDA came to the conclusion that all NSAIDs, both COX-2 selective and non-selective, raise the risk of heart disease. A study of more than 9,000 first-time myocardial infarction cases in a database showed that people who currently take diclofenac, ibuprofen, or rofecoxib have a higher risk of having another MI, but not people who currently take naproxen. Studies show that NSAIDs raise both systolic and diastolic blood pressure. This can lead to congestive heart failure and other heart problems. Several studies show that NSAIDs are even worse for cardiovascular events in people who already have cardiovascular disease or who have more risk factors for cardiovascular disease. The risk seems to depend on both the dose and the length of treatment. Higher doses and longer treatment periods are associated with a higher risk.
Gastrointestinal Complications
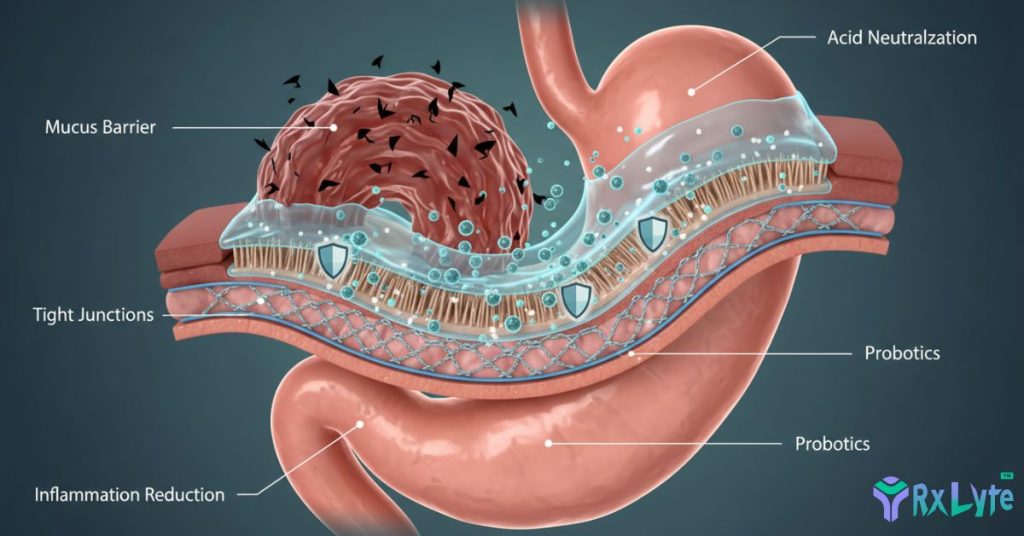
People know that NSAIDs can hurt the digestive system in a number of different ways. Medical studies show that between 2% and 4% of people who take NSAIDs for a year will develop ulcers and potentially life-threatening problems like upper gastrointestinal bleeding, perforation, and gastric outlet obstruction. By blocking COX-1 enzymes, NSAIDs reduce protective prostaglandins that maintain stomach lining integrity, increase mucus production, and regulate acid secretion. One study found that taking diclofenac increases the risk of stomach bleeding about four times compared to not taking it, while taking ibuprofen increases the risk about two and a half times. NSAIDs can cause GI problems if you are older (over 65), have a history of peptic ulcer disease, use corticosteroids or blood thinners at the same time, take higher doses of NSAIDs, or stay on treatment for a long time.
Kidney and Liver Effects
NSAIDs can impair kidney function through reduced renal blood flow, as prostaglandins help maintain adequate kidney perfusion, especially in individuals with compromised cardiovascular function or volume depletion. Prolonged NSAID use may lead to acute kidney injury, chronic kidney disease, or worsening of pre-existing kidney impairment. Regular users of NSAIDs should get blood tests that measure creatinine and estimated glomerular filtration rate (eGFR) to check on their kidney function on a regular basis. It doesn’t happen very often, but liver damage is a big problem. This is especially true for diclofenac, which has a higher risk of liver damage than other NSAIDs. Signs of liver problems include yellowing of skin or eyes (jaundice), dark urine, pale stools, persistent nausea, and upper right abdominal pain. People who already have problems with their organs should avoid or closely watch for kidney and liver problems.
Warnings and Contraindications

Some groups are more likely to get sick when they take NSAIDs, so knowing the risks and taking extra care is important for safe medication use.
Persons who should not take NSAIDs
In some situations, NSAIDs shouldn’t be used because the risks are clearly greater than the benefits:
- People who are allergic to or have hypersensitivity to NSAIDs or aspirin (for example, people with asthma, urticaria, or other allergic reactions)
- People who are having coronary artery bypass graft (CABG) surgery shouldn’t use NSAIDs to treat pain during surgery.
- People who are currently suffering from peptic ulcer disease or large intestine bleeding
- People who have very bad heart failure
- People whose livers are seriously damaged
- People who have really bad kidney disease or severe kidney impairment
If you’ve ever been allergic to any kind of NSAID, you should tell your doctor before starting any new medications, because you might be allergic to more than one kind of NSAID.
Special Populations: Women who are pregnant and children
The FDA has issued clear warnings about using NSAIDs while pregnant. The FDA says that taking NSAIDs after 20 weeks of pregnancy could hurt the unborn baby’s kidneys badly, which could lead to low amniotic fluid and other problems. A study released in 2025 shows that NSAIDs can cause problems with a fetus’s kidneys, which can lower the amount of amniotic fluid that the fetus needs to develop its lungs, digestive system, and muscles. A big study published in JAMA Paediatrics found that taking NSAIDs during pregnancy, especially indomethacin and ketorolac in the first trimester, mefenamic acid and diclofenac in the second trimester, and ibuprofen in the third trimester, was linked to a higher risk of developing chronic kidney disease as a child. When a woman is pregnant, her doctor should only give her NSAIDs after carefully weighing the risks and benefits for both her and the baby.
For kids, ibuprofen and naproxen both have dosage guidelines that are based on their body weight. Before giving NSAIDs to kids, talk to your doctor because the right dose for kids is very different from what is recommended for adults.
Health Conditions That Were There Before
Be very careful when taking NSAIDs if you have:
- Heart disease: Having a history of a heart attack, stroke, heart failure, or high blood pressure raises the risk of heart problems related to NSAIDs.
- GI problems: Crohn’s disease, inflammatory bowel disease, ulcerative colitis, or a history of peptic ulcers
- Kidney disease: Less kidney function raises the risk of NSAID toxicity and the chance of more kidney damage.
- If your liver doesn’t work right, it can slow down the breakdown of drugs and raise your risk of side effects.
- Bleeding disorders: haemophilia or other problems with clotting
- People with asthma may experience bronchospasm when they take NSAIDs.
Before starting NSAID therapy, you should always talk to your doctor about your whole medical history, especially if you plan to use them regularly or for a long time.
Interactions between drugs and lifestyle factors
Many medicines and lifestyle choices can interact with NSAIDs, which could make side effects more likely or make other treatments less effective.

Blood Pressure Medications
NSAIDs can make it much harder to control blood pressure in people who are already taking medications for high blood pressure. According to research published in medical journals, NSAIDs decrease the blood pressure-lowering effects of multiple drug classes, including angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta blockers, and diuretics. This interaction occurs because prostaglandins play important roles in regulating kidney function and blood vessel tone—mechanisms that blood pressure medications also target. The combined effect can result in elevated blood pressure, potentially precipitating heart failure or increasing cardiovascular event risk. If you already take medicine for high blood pressure, your doctor should check your blood pressure more often when you start or increase NSAID use. They may need to change the amount of medicine you take for high blood pressure as well.
Helps thin the blood and NSAIDs
Combining NSAIDs with anticoagulant (blood-thinning) medications creates a dangerous interaction that substantially increases bleeding risk. Researchers have found that taking NSAIDs with blood thinners like warfarin, apixaban, rivaroxaban, or antiplatelet drugs like clopidogrel makes the risk of serious bleeding events much higher. This interaction occurs through multiple mechanisms: NSAIDs inhibit platelet function, damage the protective stomach lining, and may enhance the anticoagulant effects of warfarin through pharmacokinetic interactions. Even selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs)—common antidepressants with mild blood-thinning properties—increase bleeding risk when combined with NSAIDs. If you need both pain relief and anticoagulation therapy, your doctor may suggest different ways to deal with pain, medications that protect your stomach, or close monitoring for signs of bleeding.
Alcohol and NSAID Use
There is a higher chance of stomach and kidney problems when you mix alcohol with NSAIDs. According to medical safety organizations, NSAIDs already carry risk of internal bleeding in the stomach, and drinking heavily may cause additional gut irritation and increase this risk. Research shows that alcohol-related ulcer risk increases when NSAIDs are consumed concurrently. Additionally, NSAIDs are linked to impaired renal function, and the National Kidney Foundation advises avoiding alcohol when taking any pain medications, as doing so may exacerbate the risk of kidney damage. People who drink very little alcohol and only use NSAIDs occasionally are not likely to have serious problems. However, people who drink a lot of alcohol and take NSAIDs regularly greatly increase their risk of medical emergencies. If you usually drink three or more alcoholic drinks every day, talk to your doctor about other ways to deal with pain before taking NSAIDs.
How to use NSAIDs safely: best practices
For the most benefits of NSAID therapy with the fewest risks and complications, it is best to follow guidelines that are based on evidence.
How to Pick the Best NSAID
Choosing the best NSAID for you depends on a number of factors that are unique to your case:
Choose Ibuprofen when:
- For serious conditions, you need pain relief that works quickly.
- You like the freedom of more frequent, shorter-duration dosing
- You don’t have any major heart disease risk factors.
- You want to find the least expensive over-the-counter option.
- You need an NSAID that is safe for kids and has been tested and proven to work.
Choose Naproxen when:
- You need pain relief that lasts longer and needs to be taken less often.
- For better sleep, you need painkillers to take at night.
- You’d rather dose only once or twice a day because it’s easier.
- You have long-term inflammatory conditions that need regular coverage.
- Further research suggests that it might be better for some patients’ hearts.
Choose Diclofenac when:
- Over-the-counter NSAIDs haven’t helped with the pain enough.
- You have very bad arthritis pain that needs stronger anti-inflammatory effects.
- For your condition, applying something topically to certain joints is best.
- Your doctor decides that the benefits are greater than the higher risk.
Minimising Risk Factors
To lower the risk of problems related to NSAIDs, try these strategies backed by evidence:
1. Use the lowest dose that works for as little time as possible to control your symptoms.
2. To keep your stomach from getting upset, take NSAIDs with food or milk.
3. Keep drinking water to help your kidneys work better while taking NSAIDs.
4. It is not recommended to take more than one NSAID (including aspirin) at the same time unless your doctor tells you to.
5. If you have GI risk factors and need long-term NSAID treatment, you might want to look into gastroprotective therapy like proton pump inhibitors.
6. Keep an eye out for signs like slurred or black stools, chest pain, shortness of breath, weakness on one side of the body, or slurred speech.
7. If you are taking NSAIDs for a long time, make sure you keep your follow-up appointments. These should include blood pressure checks and kidney function tests.
Storage and Handling
Don’t put any NSAIDs in the fridge or direct sunlight. Keep them at room temperature. Keep medicines in their original containers with labels that are still attached so that you don’t mix up different brands and strengths. NSAIDs should never be kept in medicine cabinets in the bathroom, as the humidity there can make the medicines less effective. Keep all medicines out of reach of kids by putting them in cabinets that can’t be opened. Regularly check the expiration dates on medicines and properly get rid of old medicines through pharmacy take-back programs. You should never give other people your prescription NSAIDs, because what works for your condition might not work at all for someone else.
When You Should See a Doctor
Knowing when a professional medical evaluation is needed can help avoid serious problems and make sure that the right changes are made to the treatment.
You should get emergency medical help right away if you:
- Pain, pressure, or tightness in the chest, pain that spreads to the jaw or arm, shortness of breath, and cold sweats are all signs of a heart attack.
- Suddenly feeling numb or weak (mostly on one side), being confused, having trouble speaking or understanding, having trouble seeing, getting a severe headache, or losing your balance are all signs of a stroke.
- Stools that are black or tarry, throwing up blood or something that looks like coffee grounds, and severe abdominal pain are all signs of gastrointestinal bleeding.
- In severe allergic reactions, people may have trouble breathing, their face, lips, tongue, or throat may swell, or their skin may blister or peel.
- Skin or eye yellowing, dark urine, clay-colored stools, extreme tiredness, and nausea that won’t go away are all signs of a liver problem.
If it’s not an emergency, call your doctor or nurse if:
- Pain stays the same or gets worse despite taking NSAIDs regularly.
- You’ve been in pain for more than 10 days.
- You have new or strange symptoms while taking NSAIDs.
- You have stomach problems, heartburn, or indigestion that won’t go away.
- Your legs, ankles, or feet are swollen.
- You gain a lot of weight or have trouble breathing, which are both signs of fluid retention.
- It gets harder to control, or your blood pressure goes up.
- You’re already on other medicines and want to make sure NSAIDs are safe for you.
Talking to your doctor on a regular basis will help you deal with your pain better and protect you.r health in the long run.
CONCLUSION
When used correctly, NSAIDs like ibuprofen, naproxen, and diclofenac can help a lot with pain and inflammation. But knowing the differences between them can help you make decisions that balance effectiveness with safety. Ibuprofen is easy to get over the counter, but it only lasts for a short time and needs to be taken more often. Naproxen, on the other hand, works better for longer and needs to be taken twice a day, and diclofenac is only available with a prescription and is stronger for severe pain. Each has its own risks for heart, stomach, and kidney problems. You can get the most out of your medications while minimising serious side effects by picking the lowest dose that works, taking them with food, staying hydrated, and keeping an eye out for warning signs.
Before starting regular NSAID therapy, you should always talk to your doctor, especially if you have heart disease, stomach problems, kidney issues, or take blood pressure or blood-thinning drugs. Do not take more than the maximum daily dose recommended, do not take more than one NSAID at the same time, and get medical help right away if you have chest pain, black stools, severe abdominal pain, or signs of an allergic reaction. With the right medical advice and careful attention to safety precautions, NSAIDs can be very helpful in managing your pain while also protecting your long-term health and well-being.
Frequently Asked Questions
In general, you shouldn't take more than one NSAID at the same time unless your doctor tells you to. When you take more than one NSAID at the same time, you greatly raise the risk of serious side effects like stomach bleeding, kidney damage, and heart problems, while not reducing pain any more. If one NSAID doesn't help with your pain, talk to your doctor about changing the dose or switching to a different drug instead of mixing them.
Long-term use of any NSAID is never completely risk-free, but some research suggests that naproxen may be slightly better for your heart than diclofenac and ibuprofen. On the other hand, all NSAIDs come with risks of stomach, heart, and kidney problems that get worse with longer use. Working closely with your doctor to find the lowest effective dose, using gastroprotective strategies, and keeping an eye out for early signs of complications are all things you should do if you need to manage chronic pain.
Most NSAIDs start to relieve pain 30 to 60 minutes after being taken by mouth. Because they are better absorbed, ibuprofen and naproxen sodium tend to start working a little faster. But it might take a few days of regular dosing for the full anti-inflammatory effects to show up, especially in people with long-term inflammatory conditions like arthritis. Topical NSAIDs may take longer to work because the medicine has to go through layers of skin to reach the tissues that are hurt.
Because of the higher risk of serious side effects with long-term use, taking NSAIDs every day needs close medical supervision. Medical studies show that between 2% and 4% of people who take NSAIDs for a year end up with ulcers or other problems that could be fatal. Your doctor should check to see if NSAIDs are still the best way to treat your pain every day, as well as gastroprotective drugs, regular checks on your kidney and liver function, and regular reevaluations of whether other pain management options might be safer for you.
If you already have high blood pressure, be careful taking NSAIDs because they can make it worse if you are taking blood pressure medicine. NSAIDs have been shown to raise both systolic and diastolic blood pressure. If you have high blood pressure and need to take an NSAID, your doctor should check your blood pressure more often and may need to change the way you take your antihypertensive drugs. You should never take NSAIDs without first talking to your doctor to make sure they are safe for your heart condition.
The main difference is the amount of medicine in each tablet. Ibuprofen tablets that you can buy without a prescription usually have 200 mg of ibuprofen in them. Prescription versions come in 400 mg, 600 mg, and 800 mg strengths. Two over-the-counter tablets of 200 mg each give the same total dose as one prescription tablet of 400 mg. Prescription strengths are easier to get and may be cheaper for people who need to take higher doses on a regular basis, but they are not really different medicines; they are just stronger versions of the same active ingredient.
When you put NSAIDs on your skin, like diclofenac gel, your blood levels of the drug are usually lower than when you take it by mouth. This could lower your risk of systemic side effects like stomach bleeding and heart problems. But topical NSAIDs still come with risks, especially when used on large areas of skin or for a long time. They could cause redness, itching, or rashes on the skin where they are applied. Topical NSAIDs work best on joints that are close to the skin, like the knees, hands, and ankles. They might not go deep enough to help with hip or spine problems, though.
0 Comments